The Best Ways to Fill and Fix Atrophic Scars
Compare dermal fillers, subcision, fat grafting, and biostimulators for atrophic scars. Clinical evidence on what fills depressed scars most effectively.

What Research Says About Filling Treatments
Atrophic scar filling treatments are minimally invasive procedures that restore lost tissue volume beneath depressed scars, lifting them toward the level of surrounding skin.
Quick answer — the main options for filling atrophic scars:
| Treatment | Best Scar Type | Duration of Effect |
|---|---|---|
| Hyaluronic acid filler | Rolling, shallow boxcar | 6–12 months |
| Calcium hydroxyapatite | Rolling scars | Up to 12 months |
| Poly-L-lactic acid (PLLA) | Rolling, boxcar | Up to 24 months |
| Polymethylmethacrylate (PMMA) | Rolling, boxcar | Multi-year |
| Autologous fat transfer | Rolling, broad scars | Variable |
| Subcision + filler (combined) | Rolling scars with tethering | Enhanced vs. filler alone |
Atrophic scars are depressed, indented marks that form when the skin cannot produce enough collagen during wound healing. They are the most common outcome of inflammatory acne — research indicates scarring occurs in up to 95% of acne patients. They are also caused by chickenpox, surgical incisions, and deep skin injuries.
Unlike raised (hypertrophic) scars, which result from excess collagen, atrophic scars represent a deficit of tissue. The skin heals, but the underlying structural support — collagen, elastin, and subcutaneous fat — is permanently reduced. That depression does not resolve on its own.
This is the core problem that filling treatments are designed to address.
For middle-aged adults carrying visible pitted scars from adolescent acne, this is often a long-standing frustration. The scars are permanent by nature, but clinical evidence suggests significant improvement is achievable — not through a single procedure, but through carefully selected, often combined, treatment protocols tailored to scar type, skin tone, and depth.
The sections below review what the peer-reviewed literature says about each filling approach, how they compare to resurfacing modalities, and what realistic outcomes look like.
This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare professional for diagnosis and treatment.
Atrophic scar filling treatments vocab explained:
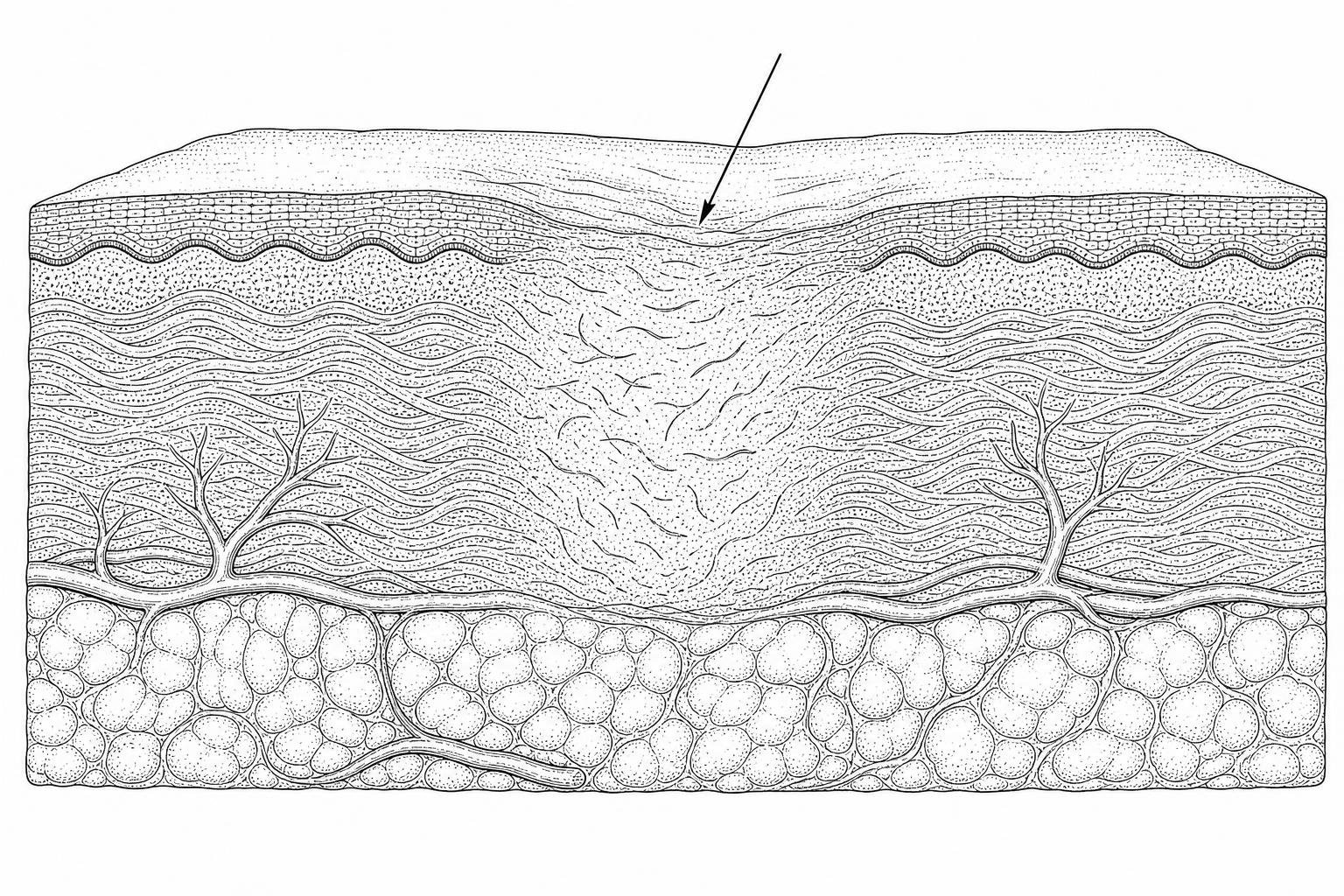
What Creates Depressed Scars
Atrophic scarring represents a failure of the skin's regenerative capacity. When an inflammatory event—such as cystic acne or a viral infection like chickenpox—damages the dermis, the body initiates a wound-healing cascade. In atrophic cases, the inflammatory mediators and enzymatic degradation of collagen fibers outweigh the production of new extracellular matrix (ECM) components.
Research published in April 2026 continues to emphasize that atrophic scars are essentially "volume-deficient" wounds. During the acute inflammatory phase, matrix metalloproteinases (MMPs) degrade the dermal framework. If the subsequent neocollagenesis (new collagen formation) is insufficient to replace the lost volume, the overlying epidermis collapses, creating a visible indentation.

Ice pick, boxcar, and rolling scars
Not all atrophic scars respond equally to atrophic scar filling treatments. Clinical assessment typically utilizes the Goodman and Baron scale to categorize scars into three primary morphological subtypes:
- Ice Pick Scars (60–70% prevalence): These are narrow (less than 2mm), deep, and V-shaped. They extend vertically into the deep dermis or even the subcutaneous tissue. Because they are so narrow and deep, standard dermal fillers are rarely effective as a primary treatment.
- Boxcar Scars (20–30% prevalence): These are round-to-oval depressions with sharp, well-defined vertical borders. They can be shallow (0.1–0.5mm) or deep (≥0.5mm). Shallow boxcar scars may respond to fillers, but deep ones often require resurfacing first.
- Rolling Scars (15–25% prevalence): These create an undulating, wave-like appearance on the skin. They are typically wider than 4–5mm and are caused by abnormal dermal-to-subcutaneous fibrous tethering. These are the "gold standard" candidates for filling treatments because they are distensible (they disappear when the skin is stretched) and lack sharp edges.
For more information on the broader scope of these indentations, see Treating Atrophic Scars: Peels, Fillers, and More.
Why acne scars leave depressions
The primary driver of atrophy is the destruction of the dermal collagen matrix. During severe inflammation, fibroblasts—the cells responsible for collagen synthesis—may become dysfunctional or undergo apoptosis. Furthermore, the loss of subcutaneous fat often accompanies deep inflammation, removing the structural "cushion" beneath the skin.
Clinical observations suggest that the degree of scarring is directly proportional to the duration and severity of the preceding inflammation. This is why early intervention in active acne is the most effective way to prevent the need for future atrophic scar filling treatments.
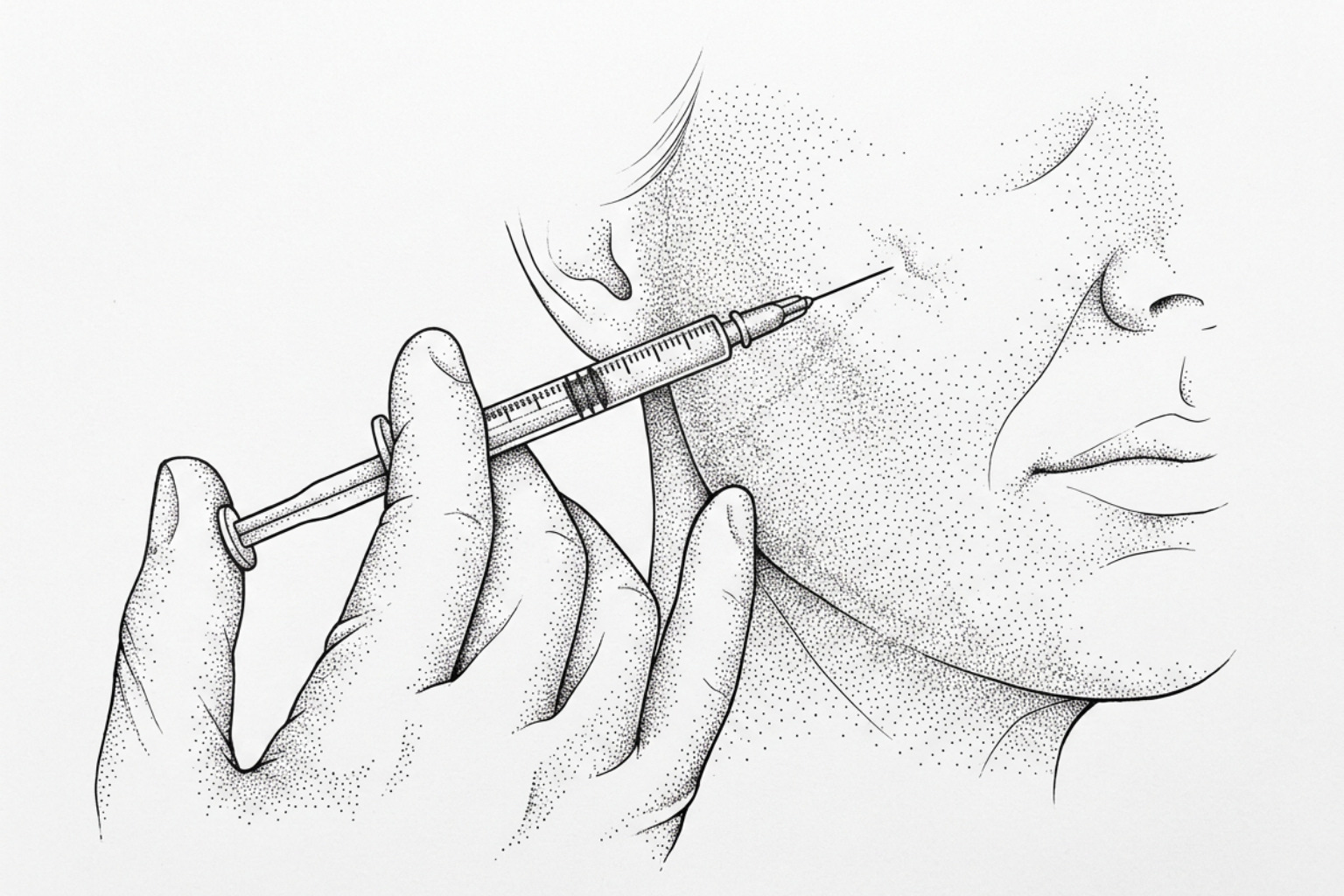
How Dermal Fillers Treat Depressed Scars
Dermal fillers, or soft tissue augmenting agents, function by providing immediate volumetric restoration. By injecting a biocompatible substance into the dermal or sub-dermal plane, clinicians can physically lift the floor of the scar. However, modern fillers do more than just "fill space"; many stimulate the body's own fibroblasts to produce new collagen over time.
A comprehensive Atrophic Postacne Scar Treatment: Narrative Review - PMC notes that while fillers provide high patient satisfaction, they are often most effective when integrated into a multi-modal plan.
Hyaluronic Acid as a Primary Agent for Atrophic Scar Filling Treatments
Hyaluronic acid (HA) is the most frequently used agent for scar filling due to its favorable safety profile and reversibility. HA is a naturally occurring glycosaminoglycan in the skin that can hold up to 1,000 times its weight in water, providing both volume and hydration.
- Mechanism: HA fillers provide structural support and have been shown in murine models to induce neocollagenesis via mechanical stretching of fibroblasts.
- Longevity: Results typically last 6 to 12 months.
- Suitability: Excellent for rolling scars and soft boxcar scars.
- Reversibility: The enzyme hyaluronidase can dissolve HA fillers if complications occur or if the aesthetic result is unsatisfactory.
For a deeper look at non-surgical options, explore our non-invasive acne scars complete guide.
Long-term Biostimulatory Fillers: PLLA and Calcium Hydroxyapatite
Biostimulatory fillers are designed to trigger a controlled inflammatory response that leads to long-term collagen deposition.
- Poly-L-lactic Acid (PLLA): Rather than providing immediate volume, PLLA acts as a scaffold. Over several months, the body replaces the PLLA microparticles with type I and type III collagen. Clinical data shows patient satisfaction rates exceeding 75% even at a 24-month follow-up.
- Calcium Hydroxyapatite (CaHA): This filler provides immediate correction due to its gel carrier, while the CaHA microspheres stimulate endogenous collagen. Studies indicate sustained improvement in rolling scars for up to 12 months.
Permanent vs. Temporary Filler Options
The choice between temporary and permanent fillers involves a significant risk-benefit analysis.
- Polymethylmethacrylate (PMMA): This is a permanent filler containing bovine collagen and PMMA microspheres. In a large study of 96 patients, PMMA resulted in a 99% improvement rate. However, because it is permanent, any complications (like granulomas or nodules) are much more difficult to treat.
- Autologous Fat Transfer: This involves harvesting fat from the patient's own body (usually the abdomen or thigh) and injecting it into the scars. While it offers the lowest risk of rejection, the "take" rate of the fat is variable, and some of the volume may be reabsorbed by the body within the first three months.
Procedures and Combination Approaches
The technical execution of atrophic scar filling treatments is as critical as the choice of material. Injecting into a scar is more complex than standard cosmetic volumizing because scar tissue is often fibrotic and resistant to expansion.

The Synergistic Effect of Subcision and Dermal Fillers
Subcision is a surgical technique used to treat tethered rolling scars. A clinician inserts a needle or cannula beneath the scar and moves it horizontally to sever the fibrotic bands that pull the skin downward.
- The Problem: If subcision is performed alone, the tethers may re-attach during the healing process.
- The Solution: Injecting a filler immediately after subcision acts as a "spacer," preventing the tethers from re-forming and providing immediate elevation.
Research in Chapter 41 Specific Attention Areas in Scar Management: Management of Atrophic Scars highlights that subcision plus HA filler significantly outperforms subcision alone in randomized trials.
Combining microneedling with energy devices
Filling treatments address volume, but they do not always address the surface texture or color of the scar. This is where combination therapy becomes essential.
- Microneedling: This creates thousands of microscopic "channels" in the skin, triggering a wound-healing response. When combined with fillers, it can improve the overall skin quality. Learn more about this at microneedling for scar reduction.
- Fractional CO2 Laser: This is often considered the gold standard for resurfacing. While fillers lift the scar from below, the laser planes down the edges from above.
- Radiofrequency (RF) Microneedling: This delivers heat into the deep dermis, tightening the skin and further stimulating collagen around the filler.
Fillers vs. Resurfacing for Depressed Scars
Patients often ask whether they should choose a filler or a laser. The answer depends on whether the primary issue is depth (volume) or texture (surface).
| Feature | Dermal Fillers | Laser Resurfacing (CO2/Er:YAG) |
|---|---|---|
| Primary Goal | Volume replacement | Surface refinement |
| Downtime | Minimal (1–2 days) | Significant (5–14 days) |
| Onset of Results | Immediate | 3–6 months (collagen remodeling) |
| Risk of PIH | Low | Moderate to High (especially skin types IV-VI) |
| Texture Improvement | Minimal | High |
For a comprehensive comparison, see the Frontiers | Advances in the treatment of acne scars review.
Laser Resurfacing vs. Injectable Augmentation
Ablative lasers (like CO2) vaporize the skin to a specific depth, forcing the body to grow an entirely new epidermal layer. This is highly effective for boxcar scars but carries risks of post-inflammatory hyperpigmentation (PIH). Injectables, by contrast, carry almost no risk of PIH, making them a safer first-line choice for patients with darker skin tones (Fitzpatrick types IV-VI).
Further details on laser options can be found in our laser treatment for scars complete guide.
Chemical Reconstruction of Skin Scars (CROSS) for Deep Pits
For ice pick scars that fillers cannot reach, the CROSS technique is often used. This involves applying a high concentration of Trichloroacetic acid (TCA)—usually 70% to 100%—focally to the base of the scar. This causes a deep "chemical burn" that triggers massive collagen production, eventually filling the narrow pit.
Clinical studies show that 100% TCA CROSS can achieve a >70% improvement in ice pick scars after 5–6 sessions. For more on chemical interventions, see the chemical peel scars complete guide.
Safety Profiles, Risks, and Patient Selection
While atrophic scar filling treatments are generally safe, they are medical procedures with potential complications.
Identifying Ideal Candidates for Tissue Augmentation
The ideal candidate has:
- Rolling or shallow boxcar scars: These respond best to volumization.
- Distensible scars: If the scar disappears when you gently stretch the surrounding skin, it is a prime candidate for filler.
- Realistic expectations: Fillers improve the appearance of scars but rarely achieve 100% "erasure."
- Stable acne: Active breakouts should be treated before scar revision begins to prevent new scars from forming.
Managing Potential Complications and Adverse Effects
Most side effects are transient and mild:
- Erythema and Edema: Redness and swelling usually resolve within 48 hours.
- Bruising: Common after subcision, resolving in 7–10 days.
- Granulomas: Small, firm lumps can form as an immune response to the filler. These are more common with permanent fillers and may require steroid injections.
- Vascular Occlusion: A rare but serious complication where filler is accidentally injected into a blood vessel. This requires immediate intervention with hyaluronidase (for HA fillers).
Frequently Asked Questions about Atrophic Scar Filling
How long do filler results last for acne scars?
For most patients, hyaluronic acid fillers last between 6 and 12 months. Biostimulatory fillers like PLLA can provide results for up to 24 months. Because the injection itself can stimulate some permanent "natural" collagen, many patients find that they need less filler in subsequent sessions.
Can fillers fix deep ice pick scars?
Generally, no. Ice pick scars are too narrow for the filler to be placed effectively. These scars are better treated with TCA CROSS, punch excision, or radiofrequency microneedling.
Is there downtime associated with scar filling?
Downtime for filler alone is minimal—usually just a few hours of mild swelling. However, if the filler is combined with subcision, you should expect bruising and swelling for 3 to 7 days.
Conclusion
The management of atrophic scars has evolved significantly by April 2026. We now understand that a "one-size-fits-all" approach is rarely successful. The most effective results come from a personalized, multi-modal strategy: subcision to release tethers, atrophic scar filling treatments to restore volume, and energy-based resurfacing to refine the skin's texture.
If you are beginning your journey toward smoother skin, a professional assessment is the first step. You can begin this process by utilizing a scar-assessment tool to identify your specific scar types and determine which clinical pathways are most likely to yield the results you seek.
Works Cited
- Attia, E. (2024). Atrophic Postacne Scar Treatment: Narrative Review. JMIR Dermatology, 7, e49954. https://pmc.ncbi.nlm.nih.gov/articles/PMC10918545/
- Gozali, M. V., & Zhou, B. (2015). Effective Treatments of Atrophic Acne Scars. Journal of Clinical and Aesthetic Dermatology, 8(5), 33–40. https://pmc.ncbi.nlm.nih.gov/articles/PMC4445894/
- Goodman, G. J. (2000). Postacne scarring: a review of its pathophysiology and treatment. Dermatologic Surgery, 26(9), 857–871. https://pubmed.ncbi.nlm.nih.gov/10971560/
- Kravvas, G., & Al-Niaimi, F. (2017). A systematic review of treatments for acne scarring. Part 1: Non-energy-based techniques. Scars, Burns & Healing, 3. https://pubmed.ncbi.nlm.nih.gov/29799567/
- Zaleski-Larsen, L. A., Fabi, S. G., & McGraw, T. (2016). Acne Scar Treatment: A Multimodality Approach Tailored to Scar Type. Dermatologic Surgery, 42(Suppl 2), S139–S149. https://pubmed.ncbi.nlm.nih.gov/27128241/